The Facts About Prostate Cancer
Could you have prostate cancer?
If
you're a man over 40 or someone in your family is, one of the most important things you can do for yourself or recommend to
that family member is to get tested for prostate cancer. Prostate cancer is the most common form of cancer in men and the
second leading cause of cancer deaths. For 1996 the projected number of new cases of prostate cancer is 317,100. This number
is expected to rise in coming years with more widespread and routine use of PSA tests for screening. Who is at risk? Almost
all men will get prostate cancer if they live long enough. The risk of developing prostate cancer increases as men get older.
Eighty percent of prostate cancer cases are diagnosed in men who are over the age of 65. However some men develop it when
they are younger. For unknown reasons, African Americans have a higher risk of developing prostate cancer than white Americans.
Asian immigrants are among those men with the lowest risk.
Get tested: Early detection pays off Prostate
cancer is usually very slow growing. Symptoms may not appear for many years. Many men will die without ever knowing they had
prostate cancer. Others will find out they have early, middle, or late stage prostate cancer.
Because prostate
cancer is so prevalent and symptoms may not exist, it is extremely important that you and male family members over 40 get
tested for the disease.
The goal of each treatment is to extend life and allow life to be lived as it always
has - remaining active, spending time with family and being part of the community.
But the definition of
successful treatment changes as the disease advances. Successfully treating early-stage prostate cancer often means curing
it. Successfully treating advanced prostate cancer means delaying its symptoms (sometimes for many years).
Awareness
is the first step to successful treatment. This booklet provides an introduction to prostate cancer and its treatment options.
It is meant to make you aware that all males are at risk; that prostate cancer is a disease you can battle and win; that patients
can lead an active life while undergoing treatment; and that testing is crucial, because you need to know you have the disease
before you can get treated.
What You Need to Know about Prostate Cancer
Where
and what is the prostate?
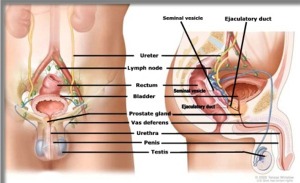
 The prostate is a gland, the size and shape of a walnut. It's located below the bladder, just in front of the rectum. Passing
through the center of the prostate is the urethra. During ejaculation, muscles surrounding the prostate squeeze the seminal
fluid into the urethra and out through the penis.
The prostate is a gland, the size and shape of a walnut. It's located below the bladder, just in front of the rectum. Passing
through the center of the prostate is the urethra. During ejaculation, muscles surrounding the prostate squeeze the seminal
fluid into the urethra and out through the penis.
The urethra also carries urine. When the prostate becomes
enlarged, it squeezes the urethra and interrupts the flow and control of urine. Consequently, one of the symptoms of prostate
cancer is urinary difficulties. Surgery, an effective treatment for the early stages of prostate cancer, can also cause urinary
difficulties.
Alongside the prostate is a group of nerves that go to the penis and control erections.
Surgery can damage these nerves, with impotence as the result. In recent years, a nerve sparing" technique has been practiced
by surgeons to help patients maintain the ability to achieve an erection. Success depends on the size and location of the
tumor. If surgery is an option for you, the chance of becoming impotent may affect your decision to undergo surgery.
Bear in mind, though, that both urinary difficulties and impotence are treatable.
What
is prostate cancer?
In any body tissue, cells normally reproduce themselves in an orderly and controlled manner;
worn out tissue is routinely replaced. Cells growing out of control form a growth, which is called a tumor. Some tumors grow,
but always stay at the same site without invading adjacent tissues, and these are called benign tumors. Other tumors not only
grow but also have the potential to invade and destroy surrounding tissue, as well as to spread to distant parts of the body.
These are called malignant tumors, or cancer. Cancer cells can detach from malignant tumors and travel to other parts of the
body and begin to grow. Tumors that develop in another organ or structure as a result of spreading in this manner are called
metastases.
What are its causes?
No one knows exactly what causes prostate cancer.
Some researchers think environmental factors, such as high-fat diets, may be the culprit; some attribute prostate cancer to
genetics. Regardless of the cause, the greatest risk factor for prostate cancer is age. The likelihood of developing prostate
cancer starts to increase after the age of 40.
Diagnosing Prostate Cancer
How
can you know if you have prostate cancer?
There are a variety of ways to detect prostate cancer. Some of these
are described below.
Symptoms of the disease:
While some patients have no symptoms,
others may experience frequent, difficult or painful urination; dribbling urine; blood or pus in the urine; or blood or pain
on ejaculation. Such symptoms may also indicate prostate problems other than cancer. To be sure, a doctor will have to perform
a thorough examination. The severity of symptoms does not necessarily relate to the severity of the tumor.
Digital
rectal examination (DRE):
In this test a gloved finger is inserted in the rectum. The physician feels for the
size, shape and texture of the prostate. Cancer feels hard. However, more tests will be needed to make sure that cancer is
present.
PSA test:
This is a blood test that measures the levels of prostate specific
antigen (PSA). PSA is a protein found in the blood and produced by the prostate. PSA levels rise in the presence of prostate
cancer. Although the test is not 100% accurate, PSAs have become an important step in diagnosing prostate cancer and following
the course of disease.
Transrectal ultrasonography (TRUS):
With a probe inserted
in the rectum, TRUS shows sound waves bouncing off the prostate and other parts of the body. It is sometimes used along with
PSAs and DREs to diagnose prostate cancer. It may also be used to help the biopsy process.
Biopsy:
This a surgical procedure in which a few cells are removed for microscopic examination. Biopsies are usually done using
a local anesthetic. The biopsy allows for an accurate assessment of the presence and types of cancer cells within the prostate.
Be on the lookout
The highest risk groups for prostate cancer are African-American
men and men with a family history of the disease. However, every man aged 40 and older is at risk. Therefore, the American
Cancer Society recommends that:
All men aged 40 and older should get a digital rectal exam (DRE)
as part of their regular, annual physical checkup.
All men aged 50 and older should get a
PSA test as part of their annual physical, in addition to a DRE.
If the DRE or PSA test is
suspicious, a transrectal ultrasound should be performed.
Remember, prostate cancer often occurs
without any symptoms. Regular testing can lead to life-saving therapy.
Stages of prostate cancer
Doctors characterize the extent of prostate cancer with what is called staging. Either of two staging systems are used.
A-through-D system:
In the early stages (A and B), only a few cells of the prostate
are cancerous and are confined to the prostate. Over time, the cancer takes over more of the prostate. In the advanced stages,
the cancer spreads to surrounding tissues (C), then to lymph nodes, other organs and the bones (D).
>TNM
system:
In this system, T stands for tumor size, N for lymph node involvement and M for degree of metastases. All designations
are included in staging. For example, T3c,Nl,M0 means that the tumor has extended into the seminal vesicles (T3c), one lymph
node is cancerous (N 1) and there is no sign of cancer in other areas of the body (MO). The TNM system corresponds closely
to the A-through-D system but not exactly.
Grading
In addition to staging, physicians
rate how life-threatening the tumor is by using the Gleason system. The biopsied tumor is put under a microscope, and the
cells are assigned a grade according to how closely they resemble normal cells. Tumors with a Gleason score of 2 to 4 contain
more normal looking cells and are generally slow growing. Tumors rated S to 10 are the most aggressive types
.
Treating Prostate Cancer
How can you treat prostate cancer?
How prostate cancer is treated depends on the stage of the cancer, the aggressive nature of the cancer, the age of the patient,
the patient's overall health, and the side effects of the different treatments. Because so many treatment options exist, your
treatment should be a carefully weighed decision involving you, your family, and your doctor.
One of the
treatment options is watchful waiting. Because prostate cancer usually grows so slowly, symptoms may not appear for years,
and men generally develop the disease late in life, a period of observation is one of your choices. Watchful waiting avoids
the side effects and discomfort caused by any treatment. However, as the disease progresses, more active treatments may seem
appropriate.
Treatment depends on the stage of prostate cancer. In early stages, getting rid of the cancer
or destroying tumor cells is the primary objective. If the cancer has reached an advanced stage, there is too much tumor to
eradicate. Therefore, the goal becomes slowing the cancer's growth.
Prostate cancer grows with male hormones
such as testosterone, which is primarily made in the testicles. Treating advanced prostate cancer depends on stopping the
male hormones from "feeding" the tumor cells. This strategy is called hormonal therapy. Recently, studies have shown
that hormonal therapy can also provide benefits in the early stages of prostate cancer.
How do
you treat the early stages of prostate cancer?
In the beginning stages, when prostate cancer is localized (confined
to the prostate), treatment options generally include:
Prostatectomy:
This is the
surgical removal of the prostate. The objective is to stop the growth of the tumor by removing the prostate. Side effects
may include impotence and difficulty controlling urination.
Radiation therapy:
This
treatment shrinks tumors that are still in the prostate either by 1) directing radiation (x-rays) at the tumor from outside
the body, or 2) implanting tiny radioactive seeds directly into the prostate. Radiation can cause impotence, diarrhea, cramps,
rectal irritation, and difficulty with urination.
The benefits of radiation therapy can be improved with
complete hormonal therapy (CHT). Recent studies have shown that patients given CHT in conjunction with radiation therapy remained
cancer-free for an average of 21 months longer than patients given only radiation therapy. CHT is the combination of two drugs,
EULEXIN® (flutamide) and an LHRH agonist (Lupron®* or Zoladex®t). The two drugs work together to stop male hormones
from "feeding" cancer cells. CHT does not add substantial side effects to radiation therapy alone.
*Lupron®
(leoprolide) is a registered trademark of TAP Pharmaceuticals Inc.
Zoladex® (goserelin acetate) is a registered trademark
of Zeneca Pharmaceuticals.
How do you treat advanced prostate cancer?
Symptoms may
not be present even in advanced prostate cancer. The goal of treating advanced prostate cancer is to slow further growth of
the disease, even before symptoms begin. Slowing the growth will delay the onset of symptoms or drastically reduce their severity.
Hormonal therapy is usually used for slowing the spread of prostate cancer.
Partial Hormonal Therapy
Most testosterone is made in the testes. With partial hormonal therapy, testes stop producing testosterone. Examples of
partial hormonal therapy include the following:
Estrogen:
Estrogen (DES) is a female
hormone that is used occasionally in the treatment of prostate cancer. When men take estrogen their testosterone levels fall.
However, the use of estrogens is limited due to their many side effects. Taken as a pill once a day, estrogen can cause nausea,
vomiting, breast tenderness or enlargement, serious heart or blood vessel problems (such as stroke, clots, fluid retention),
and lower sex drive.
Orchiectomy:
Orchiectomy is also known as surgical castration,
which is the removal of the testicles by surgery. Without testicles, the main source of male hormones is absent, which slows
the growth of the tumor. Side effects usually include impotence and hot flashes. The surgery can be performed without an overnight
hospital stay.
Medical Castration:
The ability of the testicles to make testosterone
can also be stopped without surgery. Medical castration shuts off the supply of testosterone by the testicles and achieves
the same result as surgical castration. Medical castration involves injections of Lupron®* (leuprolide) or Zoladex®t
(goserelin) once a month or once every three months. These medications are also referred to as LHRH agonists. An LHRH agonist
helps reduce the amount of testosterone similar to the surgical procedure. Side effects usually include hot flashes, impotence,
breast enlargement and tenderness, loss of sex drive, and nausea.
*Lupron® (leuprolide) is a registered
trademark of TAP Pharmaceuticals Inc.
Zoladex® (goserelin acetate) is a registered trademark of Zeneca Pharmaceuticals.
Complete hormonal therapy
While the regular injections of LHRH agonist stop the testicles
from making testosterone, they do not eliminate all testosterone in the body. A medicine called EULEXIN® (flutamide) prevents
the remaining testosterone from reaching prostate cancer cells.
The combination of LHRH agonists (Lupron®
or Zoladex®) plus EULEXIN is called complete hormonal therapy. Complete hormonal therapy virtually shuts off the body's
supply of male hormones and slows the growth of the tumor.
Prostate cancer support groups
Prostate cancer treatments can help you physically. Staying active and talking about your feelings can help you feel good
mentally. To keep a positive attitude, joining a support group may help.
In a support group you can talk
with prostate cancer patients who know exactly what you and your family are going through. In addition, support groups teach
various coping mechanisms for stress, depression and anxiety. Many prostate cancer patients have greatly benefitted from support
groups.
The organizations listed below provide support for men with prostate cancer and their families.
You can call them for details about their organization.
US-TOO
930 North York Road, Suite 50
Hinsdale,
IL 60521-2993
Tel: 800.80-USTOO
Patient Advocates for Advanced Cancer Treatments (PAACT)
1143
Parmelee, NW
Grand Rapids, MI 49504
Tel: 616.453.1477
American Cancer Society, Inc.
1599
Clifton Road, NE
Atlanta, GA 30329-4521
Tel: 800.ACS.2345
Local chapters of the ACS provide
literature, counseling, and guidance for cancer patients and their families. The ACS sponsors a number of programs, including:
CanSurmount, which brings together patients or families with trained volunteers who can provide one-on-one
help.
I Can Cope, an 8-week course that addresses practical and emotional needs of people with cancer.
American Foundation for Urologic Disease
300 W. Pratt St.
Baltimore, MD 21201
800.242.2383



 Many men worry about whether surgery for benign prostate hyperplasia (BPH) will affect their ability to enjoy sex. Some sources
state that sexual function is rarely affected, while others claim that it can cause problems in up to 30 percent of all cases.
Many men worry about whether surgery for benign prostate hyperplasia (BPH) will affect their ability to enjoy sex. Some sources
state that sexual function is rarely affected, while others claim that it can cause problems in up to 30 percent of all cases.


